New guideline from the
Infectious Diseases Society of America (IDSA) recommend that physicians should
prescribe antibiotics only for patients with sore throats who have positive
test results for a group A streptococcal (GAS) infection.
The recommendations include:
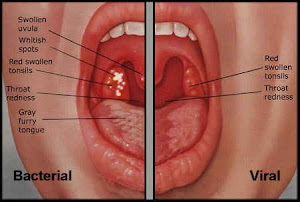
1. Because the clinical features alone do not
reliably differentiate between GAS and viral pharyngitis swabbing the throat
and testing for GAS by rapid antigen detection test (RADT) and/or culture
should be performed except when clear viral features like rhinorrhea, cough,
oral ulcers, and/or hoarseness are present. In children and adolescents (and
not in adults), negative RADT tests should be backed up by a throat culture.
2. Diagnostic studies for GAS pharyngitis are generally
not indicated for children <3 years old and adults because acute rheumatic
fever is rare in these groups.
3. Routine follow-up throat
cultures or RADT are not generally recommended.
4. Diagnostic testing or
empiric treatment of asymptomatic household contacts of those with acute GAS
pharyngitis is not routinely recommended.
5. Those with acute GAS pharyngitis should be
treated with an appropriate antibiotic at an appropriate dose for duration likely
to eradicate the organism. Ten days treatment with penicillin or amoxicillin is
recommended for those non-allergic to them.
6. Treatment of penicillin-allergic patients include a first generation cephalosporin (for
those not anaphylactically sensitive) for 10 days, clindamycin or
clarithromycin for 10 days, or azithromycin for 5 days.
7. Adjunctive therapy with analgesic/antipyretic
agent may be useful in the management of GAS pharyngitis. Corticosteroid is not
recommended and aspirin should be avoided in children.
8. GAS carriers do not generally require
antimicrobial therapy because they are unlikely to spread GAS pharyngitis to
their close contacts and are at little or no risk for developing suppurative or
nonsuppurative complications.
9. Tonsillectomy is not recommended solely to
reduce the frequency of GAS pharyngitis.

No comments:
Post a Comment